





Today we’d like to introduce you to Mary Medeiros.
So, before we jump into specific questions about the business, why don’t you give us some details about you and your story.
I was essentially groomed by my parents — both physicians… prison psychiatrists actually — to be a doctor from the time I was a little kid. I understood it to be a default career path, so in college I majored in Music because I figured it would be my last chance to focus on something I really loved! With my music degree and med school prerequisites in hand, I went on to Loma Linda University in California to get my M.D.
During my 3rd-year Surgery rotation I saw a patient in clinic with a severe diabetic foot infection. It was my job that day to deal with his foot, possibly planning for amputation, but he had no primary doctor to manage his poorly controlled diabetes, which didn’t sit well with me. It was suddenly clear that what I wanted was to care for the whole patient and I had in mind to provide primary care in some underserved environment someday.
I came back East for Internal Medicine residency followed by a second board certification in Preventive Medicine with a correctional (prison) health track, earning a Masters of Public Health (MPH) along the way. But now married with our first child on the way, I rerouted to working exclusively in the hospital at UMass in Worcester, mostly doing night shifts. Office hours seemed more feasible once my eldest approached school age and at last I transitioned to a position in the field of Primary Care, but it didn’t take long in a corporate group practice setting to feel crushed by the increasing administrative tasks that get in the way of caring for patients.
I hit a point of burnout that is accelerating to an alarming rate of prevalence amongst Primary Care docs. Depending on where they are in their careers and lives, some of my colleagues respond by retiring earlier than they might have, some transition to jobs that don’t involve patient care like administrative positions, education, medical writing, research, and so on.
Me… I pulled the plug and submitted my resignation without a plan which felt quite unsettling, because I am hard-wired to be driven and had been so focused on medicine for so long that it was difficult to imagine walking away and never coming back. While exploring options online, I discovered Direct Primary Care and it sounded simply too good to be true. But I kept reading and searching and was shocked to discover that doctors are indeed doing it and not only succeeding, but feeling passionate about practicing medicine again, while enjoying their lives. So I went for it.
Overall, has it been relatively smooth? If not, what were some of the struggles along the way?
Building a Direct Primary Care practice has been quite a ride, but I don’t regret it in the least. It is widely understood that physicians are terrible business-people. Think about it: in the past 15 years, work hours for interns and residents had to be *limited* to 80hrs/week. Meanwhile, the average salary for a resident has been roughly $50K/yr. If you do the math, that amounts to roughly $13/hr., which is less than what I currently pay my administrative assistant, but it involves quite literally taking the responsibility of people’s lives in your hands while in the midst of a 30hr shift every 4th night. When you spend several years in that culture, you start expecting to give away your labor, no matter how high-risk the task. Salaries for doctors vary extremely widely, but it turns out because of the way value is calculated for physician labor, across the board the lowest paid positions are primary care and psychiatry. Is it any wonder that there are shortages of doctors in these fields?
What I have come to learn in the process of pursuing a Direct Care model of medical practice, is that connecting the dots between what people are willing to pay (the dollar value) and the actual cost and perceived importance (market value) of a medical service are completely enshrouded by the third party reimbursement system, or what we have come to know as “health plans.” People don’t know what the services cost but have been trained by this system to believe it “should” cost “nothing” since they have already paid for it in insurance premiums and taxes. The reality is that, first of all, obviously it does not cost nothing to provide medical services since there are facilities that need to be maintained, salaries of support staff that need to be paid, equipment and supplies, etc., etc. Meanwhile, prices charged for a given service are manipulated by people who DO have good business sense — which are generally not front-line medical providers — and negotiated with carriers of health plans who then, theoretically, pay on behalf of patients. But frankly these health plan carriers are hiking premiums and deductibles through the roof in order to cover the costs incurred for services provided to patients. This is only clogging the system further because patients perceive going without insurance as either risky or illegal or both, and basically feel trapped, obligated to pay outlandish premiums that make no sense, especially to those who are fairly healthy thereby hardly using the medical system at all.
The irony of my style of practice is that most people will take one look, see my fees as an “extra” medical cost, and assume I’m falling in line with every other piece of the health care industry that seems to be taking them for a ride. However, when it becomes clear that I don’t earn any money outside of the published fees — not one dime comes into my practice from any health plan at all including Medicare or MassHealth [Massachusetts Medicaid] — the script completely changes with people asking how I can stay afloat in my practice charging as little as I do for the level of service I provide. It is often an educational hurdle to bring people to that point of understanding, particularly in Massachusetts where universal health care coverage is mandated and covered providers are still relatively robust compared to other areas of the country.
Meanwhile, the operations of a Direct Primary Care practice are utterly distinct from other medical clinics because the revenue stream gets no help from third parties like insurances, so I find myself falling more in line with other direct pay service providers like contractors, fitness clubs, financial advisors, etc., where as a solo provider I have to start lean to keep overhead low, meaning I have had to learn to manage the business operations myself. Unlike typical medical practices who have business funneled to them by insurance plans they contract with to automatically send them patients, growth of my practice depends on networking and reputation, since I don’t really have much of a budget for marketing. It’s a lot of hats to wear.
Please tell us about Thrive Adult Primary Care.
Thrive Adult Primary Care is a young endeavor, less than a year old. You have heard me referring to it as a Direct Primary Care practice, which is a brand new concept for most people. I have a fairly well-developed set of visual aids with fun graphics that I use to help pull the concepts together, but I’ll do my best to break it down using words alone.
In short, I say Direct Primary Care is a *relationship* between a doctor and patient that is unencumbered by the increasing complications of the third party reimbursement system, whereas third parties are health insurance carriers and government-funded health plans. When these plans provide the payment, they also control what patients have access to for care. In Direct Primary Care, there is a periodic membership payment to retain the doctor-patient relationship, and it basically passes through no other hands than that of the patient and the doctor. This frees up the doctor to take care of the patient in accordance with his or her professional training and expertise, rather than being enslaved by checklists on the computer in the form of billing, coding, tracking measures and so forth. I like to say I am no longer employed by insurance companies — instead, I am exclusively employed BY MY PATIENTS.
People most commonly ask one of two questions next.
A very common question is, “So I don’t need insurance?” The answer is YES, you do need insurance; it’s just that your insurance doesn’t pay *me*. Just as you need insurance for your car while you pay out of pocket to get oil changes done by a mechanic. Your car insurance and your mechanic are not directly connected, if they are connected at all. Direct Primary Care separates out routine prevention and maintenance from what “insurance” was originally meant to be for, which is to protect a patient’s assets in case of a catastrophic event. The concept of health insurance has gotten far, far away from this and needs to be re-evaluated.
The other common question asked is more a statement of assumption: “Oh, so you’re a concierge medicine practice…?” The answer is NO, Direct Primary Care and Concierge Medicine are not the same thing, although the differences from the patient perspective can be subtle and confusing. Both types of practices provide highly personal and attentive care and streamlined access so patients can often reach their own doctor around the clock, for example. But concierge practices typically cost upwards of $3000-5000 per year in retainer fees, then also bill insurances for services rendered, such as for each office visit. Direct Primary Care does not bill insurance at all for any reason, and often costs a patient less than $1000 per year, more typically averaging $80/month depending on the patient’s age.
Again, once someone gets a chance to see this clearer picture of the differences, a common question is “How can you make any money like that?” The answer is VERY CAREFULLY. As the practice is in its early stages, I am more highly focused on ensuring each new patient receives top-quality attention than on exploding the size of the patient panel. It excites me that I have the freedom now to do things like home visits or telemedicine-style care such as video chats and remotely tracking health measures like blood pressure or pedometer steps, as well as the freedom to volunteer in my kids’ classes from time to time, for example, because I can manage my own schedule. My patients are happy, because I’m happy, which helps me be more present with them and responsive to them in their times of need.
I can tell you with confidence that I am not ever going to make millions of dollars, and it will be a good couple of years before I can even pull a salary at all. But my work-life balance and job satisfaction are already eons better than any other point in my career, which is simply priceless.
If you had to go back in time and start over, would you have done anything differently?
Ha, my husband just asked me this question, as I approach the one-year mark since opening. I wish I had taken a little more time to plan and prepare. If I had been able to network sooner with other doctors doing this style of practice, I would have structured things a bit differently from the beginning. Instead, I wound up changing certain things a few months after opening the doors, mostly tech stuff like my electronic medical record system and my fax program, etc. That said, a lot of it is in better shape now, so ultimately, no regrets!
Pricing:
- Our pricing scheme can be found at this link: http://www.thriveapc.com/services-pricing/
Contact Info:
- Address: 835 West Central St, Suite 4
Franklin, MA 02038 - Website: http://www.thriveapc.com/
- Phone: 774-318-4205
- Email: info@thriveapc.com
- Instagram: https://www.instagram.com/thriveapc/
- Facebook: https://www.facebook.com/thriveapc/
- Twitter: https://twitter.com/ThriveAPC




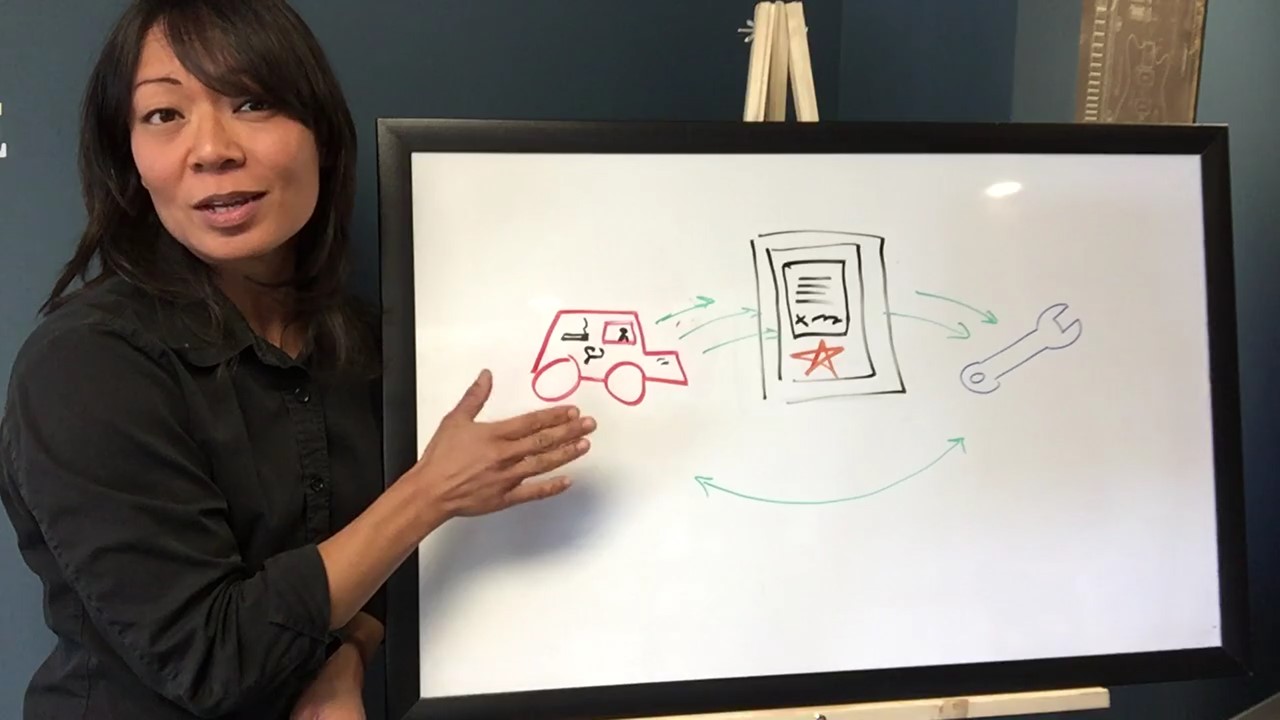



Image Credit:
Charlie Pasewark
Getting in touch: BostonVoyager is built on recommendations from the community; it’s how we uncover hidden gems, so if you know someone who deserves recognition please let us know here.











